FROSTBITE
Frostbite is injury due to formation of ice crystals within tissues. Adjacent tissues may be damaged by vasoconstriction, thrombosis, and inflammation,
Determining the severity of a cold injury can be challenging during early phases. Initial signs and symptoms in severe frostbite may appear deceptively benign; conversely, mild cold injuries such as frostnip may present similarly to frostbite.
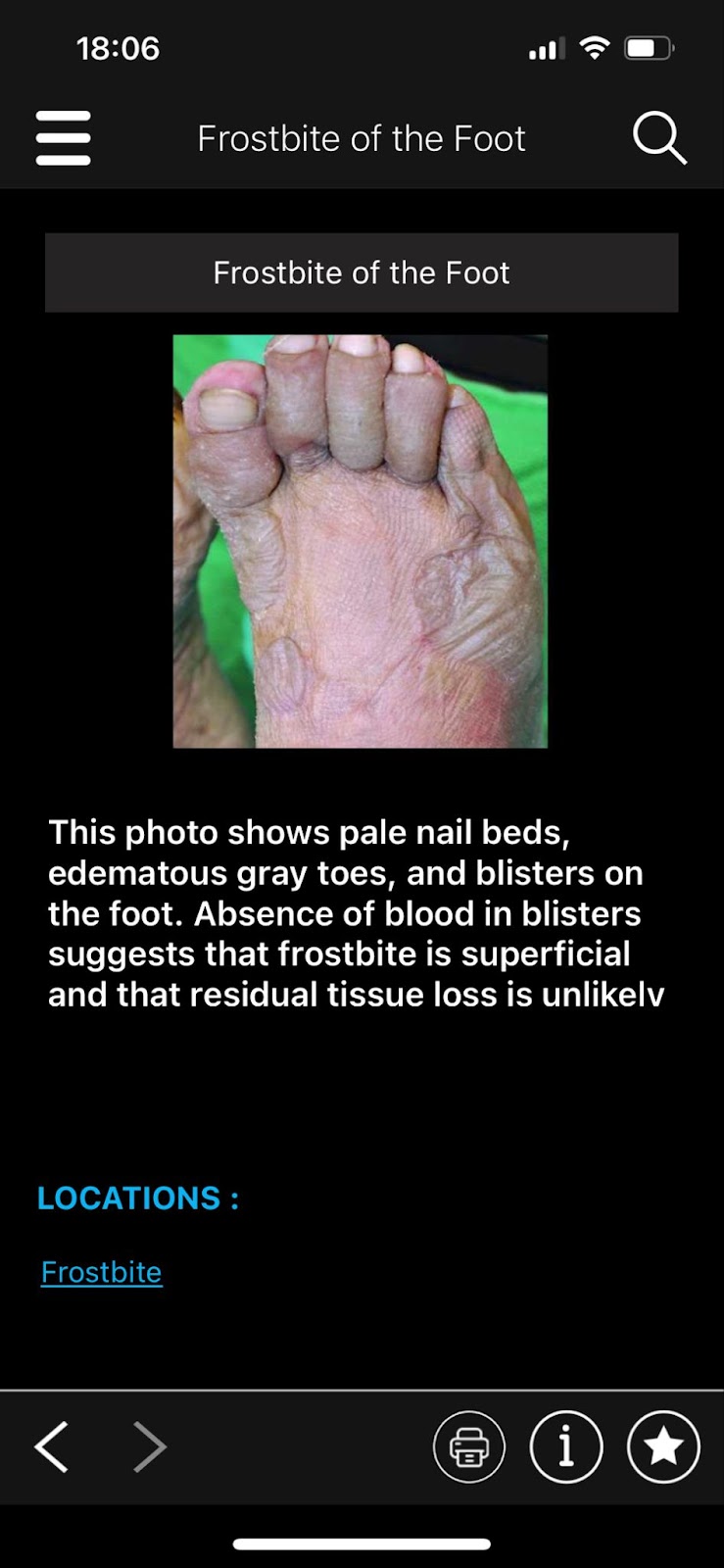
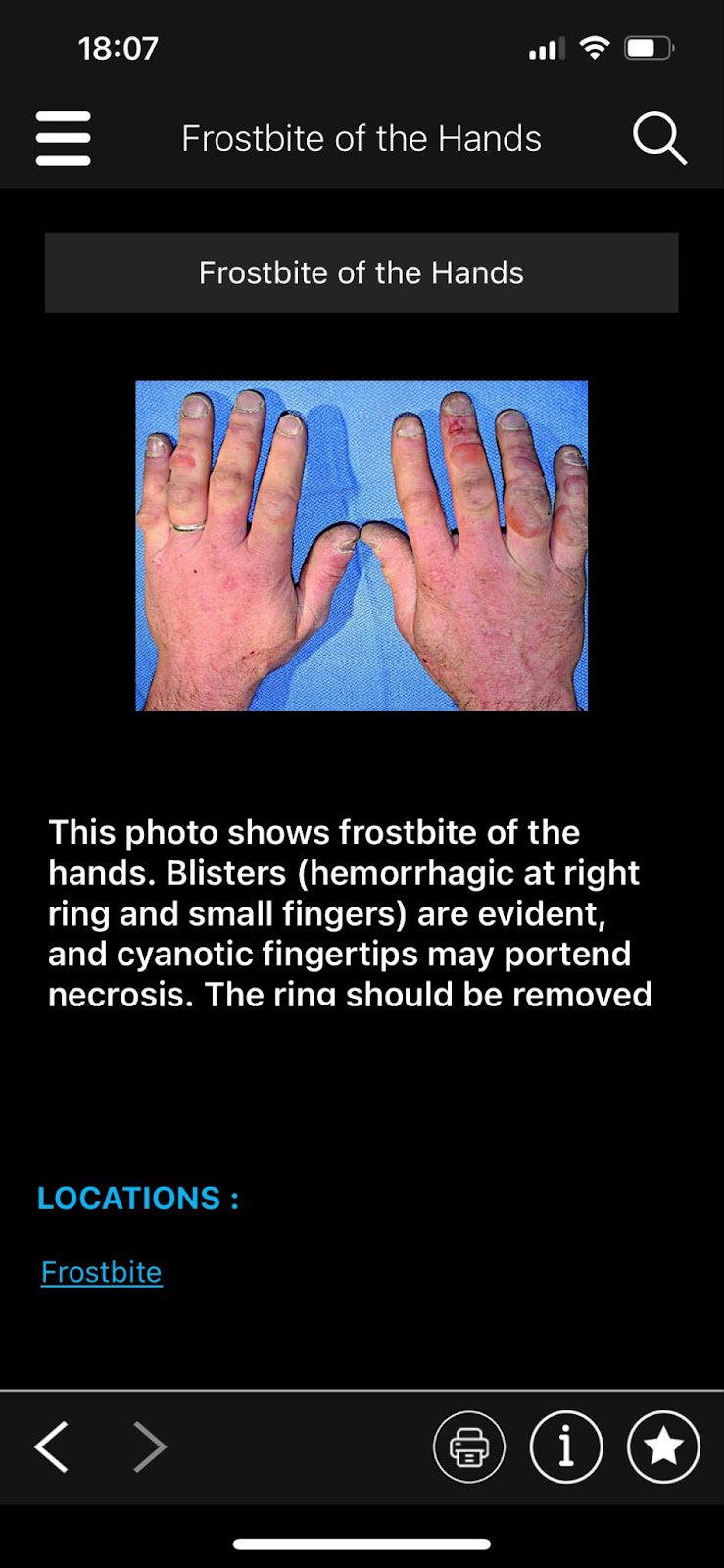
Prior to rewarming, frostbitten tissues are cold, white, hard,, numb, and sometimes blistered. After rewarming, skin becomes blotchy red, swollen, and extremely painful. Blisters tend to appear within 4-6 hours of rewarming. Clear, serum-filled blisters indicate superficial damage, without residual tissue loss, while blood-filled blisters accompany deep tissue damage and likely tissue loss. Longer-term complications can include compartment syndrome, gangrene (usually dry, with a hard black carapace over healthy tissue), need for amputation, and long-term neuropathic symptoms. The full extent of frostbite damage may take several days to several weeks to become clear.

TCCC has four frostbite categories:
First Degree (Superficial): Superficial skin injury, pain on rewarming, numbness, hyperemia, occasionally blue mottling, swelling and superficial desquamation (after ~5 days)
Second Degree (Superficial): Partial thickness injury to skin, in addition to first degree findings, vesiculation of the skin surrounded by erythema and edema (appears around day 2)
Third Degree (Full Thickness): Entire thickness of skin extending into subcutaneous tissue, bluish to black and non-deformable skin, hemorrhagic blisters, vesicles may not be present, eventual ulcerations can be expected, area will likely be surrounded by 1st or 2nd degree injury
Fourth Degree (Full Thickness): Similar to third degree, but full thickness damage including bone. Area may be cold to touch and may feel stiff or woody.
Immersion Foot (image below): Caused by prolonged exposure to moisture. Feet, especially soles, become water-logged, hyperemic, mottled, painful, and edematous, gradually progressing to blistering, hypoperfusion, ulceration, and gangrene if untreated. Treatment is re-warming and drying at room temperature. Pain control and debridement may be required. As with other cold injuries, persistent life-altering symptoms may occur.

TCCC frostbite treatment protocols are as follows:
***Treatment protocols in Ukraine will depend on local guidelines***
Address major trauma and hypothermia before focusing on frostbitten extremities.
The core of frostbite treatment is rapidly rewarming the frostbitten area in warm water (37-40 degrees celsius) This should take 15-30 min if water is kept continuously at 37-40. (TCCC calls for 40-42 degree water; however recent studies have shown this causes additional pain without improving outcomes). The longer the tissue remains frozen, the greater the damage. A general rule of thumb is that if the patient cannot reach a hospital in the next two hours, field rewarming should be undertaken. However, NEVER THAW tissue unless it can be guaranteed that it will not re-freeze. Do not thaw feet if the patient will have to walk on them in the near future; thawed tissue is delicate and susceptible to trauma. Dry heat sources should be avoided; they may burn numb tissue. Avoid the temptation to prematurely end rewarming due to pain; rapid rewarming is more painful but produces better outcomes than slow rewarming. Liberal use of pain medication is highly encouraged during the rewarming process. The patient should move the affected part gently during rewarming. Do not rub affected areas, or apply snow or oil. Leave blisters intact to prevent infection and deep tissue dessication. Preventing infection is paramount. The hospital may use vasodilators, anticlotting meds, NSAIDs, and elevation to encourage reperfusion Patients should avoid vasocontrictors such as nicotine, and be monitored for electrolyte abnormalities. Acute, persistent pain will generally subside within the first three days, although intermittent nerve pain may continue for an extended period.
No comments:
Post a Comment